PRP vs Gel vs Steroid Knee Injections
Which Treatment Is Best for Your Chronic Knee Pain?
Knee injections deliver medication or biologic substances directly into the joint to decrease pain, reduce inflammation, and improve function, especially when pills, physical therapy, and activity modification are not enough. They are commonly used for osteoarthritis (“wear‑and‑tear” arthritis), inflammatory flares with swelling, and some chronic tendon or cartilage-related problems around the knee.
Steroid (Cortisone) Knee Injections

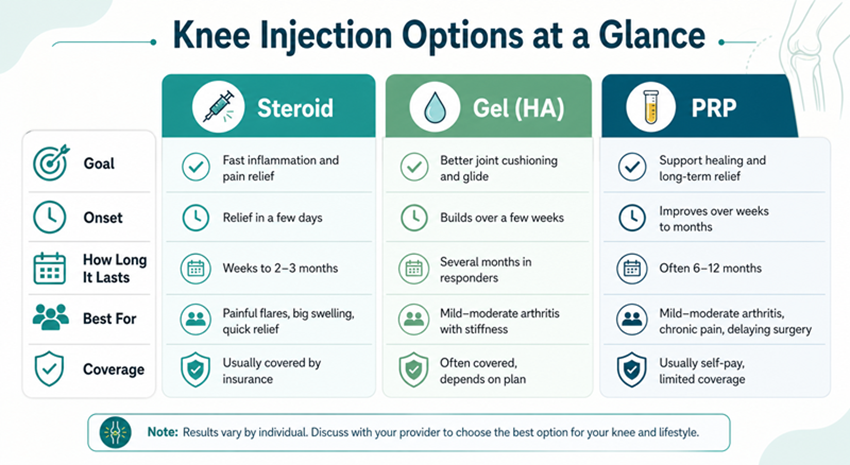
Steroid injections (corticosteroids or “cortisone shots”) deliver a strong anti‑inflammatory medicine into the knee to quickly calm inflammation and pain. They have been used for decades and are widely available, often covered by insurance.
How they work
- Corticosteroids suppress inflammatory chemicals inside the joint, which decreases swelling, warmth, and pain.
- Relief typically starts within a few days and can be quite dramatic in the short term.
How long relief lasts
- Many patients feel significant benefit for several weeks, and some get relief for up to 2–3 months after a single injection.
- Studies comparing steroid to hyaluronic acid suggest steroids win for early, fast relief, but their advantage fades after the first couple of months.
Who steroid injections are best for
Steroid injections are often a good option if:
- You have a painful arthritis flare with visible swelling and need rapid pain relief to walk, sleep, or complete an event (e.g., travel, important life events).
- You have more advanced arthritis with significant inflammation and need short‑term relief while you explore longer‑term solutions (weight loss, bracing, surgery planning).
- You cannot take or tolerate anti‑inflammatory pills due to stomach, kidney, heart, or blood‑thinner issues.
Limitations and considerations
Repeated steroid injections may carry risks, including potential cartilage damage if done too frequently, which is why many specialists limit them to a few times per year in the same joint.
Steroids treat inflammation and pain, but they do not rebuild cartilage or reverse the underlying osteoarthritis.
Hyaluronic Acid (“Gel”) Knee Injections

Hyaluronic acid (HA) injections, often called “gel shots” or viscosupplementation, add a thick, gel‑like substance to the joint to improve lubrication and cushioning. HA is similar to the natural fluid already present in a healthy knee.
How they work
- HA injections aim to restore the knee’s “shock absorber” and smooth gliding, which can ease stiffness and reduce friction-related pain.
- They do not work instantly; pain relief tends to build gradually over several weeks as the joint environment improves.
How long relief lasts
- Many patients who respond notice benefits for several months, often longer than a single steroid shot, though results vary.
- Reviews suggest HA can provide moderate improvements in pain and function for knee osteoarthritis, but it is often less robust than PRP over the long term.
Gel injections are often a good fit if:
- You have mild to moderate osteoarthritis with stiffness and activity‑related pain rather than constant severe pain.
- You are looking for non‑surgical, medium‑term symptom relief and can wait several weeks for full effect.
- You prefer an option that is often covered by insurance plans, making it more affordable than PRP for many patients.
Limitations and considerations
- Not everyone responds to HA; some patients notice little change even after a full series.
- HA improves lubrication and shock absorption but, like steroids, it does not regrow cartilage or “cure” arthritis.
Platelet-Rich Plasma (PRP) Knee Injections
PRP uses a small sample of your own blood, spun in a centrifuge to concentrate platelets and growth factors, then injected into the knee. The goal is to harness your body’s natural healing responses rather than just masking symptoms.
How they work
- Platelets release growth factors that can modulate inflammation and support tissue repair in cartilage, ligaments, and other joint structures.
- Pain relief tends to come on gradually over several weeks and may continue to improve for months as the biologic effects build.
How long relief lasts
- A number of randomized trials and meta‑analyses show PRP often provides greater and longer‑lasting improvements in pain and function than steroid or HA injections for knee osteoarthritis.
- Some studies report meaningful relief lasting 6–12 months after a PRP series, outperforming corticosteroids after the early weeks and edging out HA at longer follow‑ups.
For example:
- A 2023 network meta‑analysis found PRP and PRP plus HA were the most successful treatments for improving pain and function at 3, 6, and 12 months compared with corticosteroids, HA alone, and placebo.
- A 2025 review of 11 randomized trials reported that PRP showed the greatest and most durable improvements in knee pain and function compared with steroid or HA for osteoarthritis.
PRP is often considered for patients who:
- Have mild to moderate osteoarthritis or chronic knee pain that has not responded well to standard measures like NSAIDs, physical therapy, or prior injections.
- Are younger or active and want to delay or avoid knee replacement, and are open to biologic treatments even if they are self‑pay.
- Have certain soft‑tissue injuries (like some meniscus or tendon problems) where stimulating healing is a key goal, not just pain control.
Limitations and considerations
- PRP is usually not covered by insurance and is more expensive up front than steroid or HA injections.
- Not all PRP is the same; protocols vary (number of injections, platelet concentration, inclusion of white blood cells), and this can influence results.
While many studies are promising, PRP is still considered a regenerative or biologic therapy, so it should be done by clinicians experienced in both knee pathology and injection techniques.
What the Research Says
When looking at the big picture:
- Steroids and HA can be roughly similar in pain relief around the 3‑month mark, but the fastest early benefit usually comes from steroids.
- PRP injections frequently rank highest for both pain relief and functional improvement at 6–12 months in comparative trials for knee osteoarthritis.
- Some newer data suggest combination strategies (such as PRP plus HA, or a steroid plus HA in the same session) may blend quick relief with longer‑term benefit.
Because individual responses vary, the “best” injection is less about the product and more about matching the right treatment to the right knee at the right time.
How Our Clinic Helps You Choose
For patients in our clinic, we typically start with a detailed evaluation of:
- Your diagnosis (x‑rays, MRI if needed) and arthritis severity.
- Your symptoms (pain location, stiffness, swelling, instability).
- Your goals (stay active, delay surgery, return to sport, get through an upcoming trip).
- Your medical history and preferences, including insurance and budget.
From there, we might recommend:
- Steroid injection if you are in a significant flare and need fast relief to get moving again.
- Hyaluronic acid gel injections if you have mild to moderate arthritis, want to avoid frequent steroids, and are looking for smoother joint motion over months.
- PRP injections if you want a biologic, longer‑lasting option, especially if prior steroid or gel shots did not provide enough relief or if you are trying to postpone surgery.
Our team can also discuss whether a combination approach (for example, a short‑term steroid plus longer‑term HA or PRP plus HA) makes sense for your specific situation based on current evidence.
If you are dealing with chronic knee pain and wondering which injection is right for you, the next step is a personalized consult where we can review your imaging, examine your knee, and help you decide on a plan tailored to your goals.


