Shoulder Anatomy & Function
Understanding how your shoulder works is the first step toward preventing injuries and recovering from pain. The shoulder is one of the most complex and flexible joints in the body. It provides a wide range of motion that allows you to reach, lift, throw, push, and pull—but this versatility comes with a greater risk for injury and dysfunction.
Bones of the Shoulder
The shoulder consists of three main bones:
- Humerus: The long bone of the upper arm.
- Scapula (shoulder blade): A flat bone anchoring the upper arm and giving attachment to important muscles.
- Clavicle (collarbone): Serves as a strut between the shoulder blade and the sternum, stabilizing the entire arm.
Together, these bones create four functional joints:
- Glenohumeral Joint: The “ball-and-socket” where the rounded head of the humerus sits within the shallow glenoid cavity of the scapula. This joint supplies most of the shoulder’s movement—and is a common site for instability.
- Acromioclavicular Joint: Connection between the acromion (top of the scapula) and the clavicle. Important for raising the arm above the head and absorbing impact.
- Sternoclavicular Joint: Where the clavicle meets the breastbone. Though small, it plays a crucial role in moving the shoulder through space.
- Scapulothoracic Articulation: Technically not a true joint, but rather the way the flat back of the scapula slides across the thoracic (chest) wall, helping to lift and rotate the arm.
The glenoid labrum, a ring of cartilage around the glenoid cavity, deepens the socket and stabilizes the ball of the joint. Articular cartilage and bursae allow for smooth movement and lessen friction during motion.
Joints and Stability
While the shoulder’s bony architecture supports remarkable mobility, true stability is achieved through soft tissue structures—ligaments, tendons, muscles, and the joint capsule.
- Glenohumeral Ligaments: The superior, middle, and inferior ligaments reinforce the capsule and prevent excess movement.
- Acromioclavicular & Coracoclavicular Ligaments: Secure the clavicle to the scapula, preventing separation and injury.
- Coracoacromial Ligament: Forms an arch above the shoulder, preventing upward displacement of the humerus head.
- Joint Capsule: Thickened fibers surround the ball-and-socket joint, winding up during abduction and external rotation to provide additional stability and limit range at the joint’s extremes.
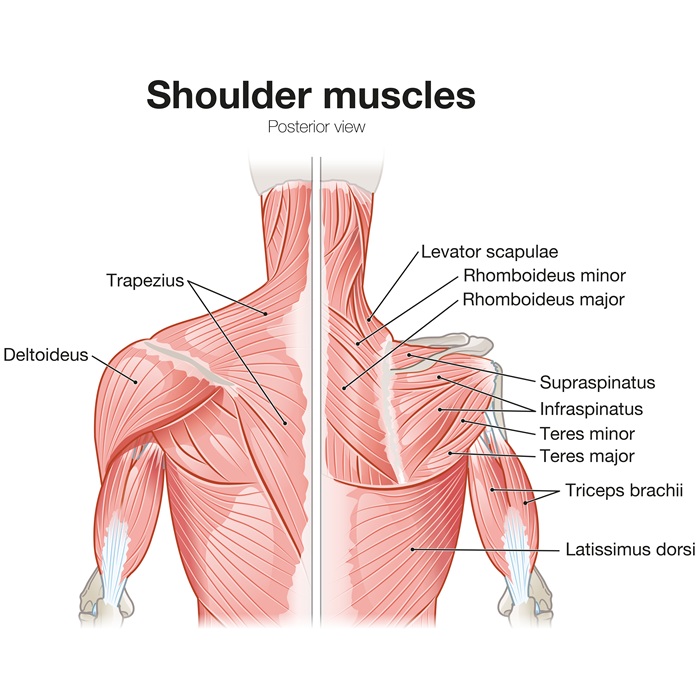
Shoulder Muscles & Soft Tissue Structures
Muscles both move and stabilize the shoulder. They’re separated into two key groups: the rotator cuff and the scapular stabilizers
Rotator Cuff
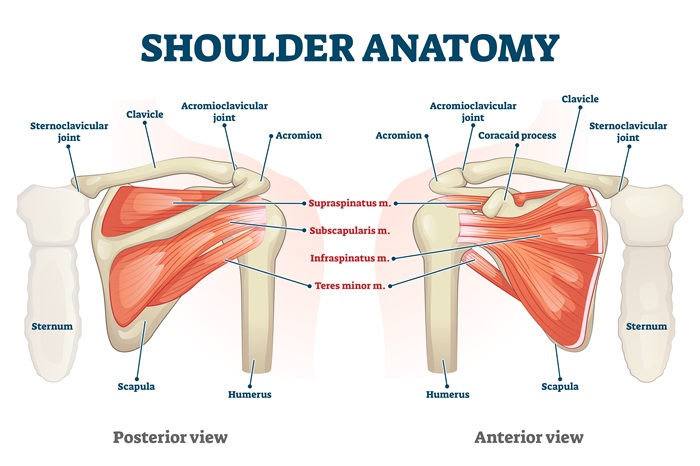
Four small muscles whose tendons blend together to form a cuff-like support around the glenohumeral joint:
- Supraspinatus: Initiates arm raising
- Infraspinatus: Provides external rotation
- Teres Minor: Also helps rotate the arm outward
- Subscapularis: Internally rotates the arm
- These muscles compress the head of the humerus into the glenoid cavity for stable movement. Damage to any rotator cuff tendon can cause pain, weakness, and reduced motion.
Scapular Stabilizers & Movers
- Deltoid: Main mover for arm abduction and lifting.
- Trapezius, Serratus Anterior, Levator Scapulae: Control the position and movement of the shoulder blade. Proper scapular rhythm is essential for healthy mechanics.
- Pectoralis Major & Minor: Aid in adduction, internal rotation, and arm elevation.
Ligaments and Tendons
Connect muscles to bones and hold joints together during movement. The biceps tendon, especially its long head, also plays a crucial stabilizing role inside the shoulder.
Nerves & Blood Vessels
The shoulder’s range is unmatched:
- Flexion/Extension: Forward and backward arm movement
- Abduction/Adduction: Lifting arm to the side and back toward the body
- Internal/External Rotation: Turning the arm in and out
Circumduction: Full-circle motion at the shoulder
Each motion involves complex coordination between the bones, joints, muscles, and soft tissues. For example:
- The rotator cuff keeps the humeral head centered as the larger deltoid moves the arm.
- The scapula rotates, tilts, and slides, driven by its stabilizer muscles, to “clear space” for the head of the humerus.
- Proper biomechanics prevent pinching and excessive wear; even minor imbalances can lead to pain and injury over time.
Shoulder Movement & Biomechanics

Common Mechanisms of Shoulder Injury
Muscles both move and stabilize the shoulder. They’re separated into two key groups: the rotator cuff and the scapular stabilizers
Acute Trauma
- Falls on an outstretched arm (FOOSH): Can fracture the clavicle or humerus, dislocate joints, or tear ligaments.
- Direct blows or impact sports: May disrupt the acromioclavicular joint or cause contusions deep within the shoulder.
- Dislocations: The humeral head is forced out of the glenoid socket, often damaging the labrum and ligaments.
Overuse & Repetitive Motion
- Impingement Syndrome: Frequent overhead activities or poor mechanics lead to pinching of rotator cuff tendons between the humeral head and acromion.
- Tendinitis & Bursitis: Chronic abrasion or overload causes inflammation or swelling, impeding smooth movement and producing pain.
- Labral Tears: The cartilage ring can be damaged by twisting or pulling motions, especially during throwing or lifting.
Degenerative Changes
- Osteoarthritis: Cartilage wears away with age or excessive use, creating pain and stiffness.
- Rotator Cuff Degeneration or Tears: Over time, tendons fray, thin, and sometimes rupture.
Other Common Injuries
- Fractures: Of the clavicle, humerus, or scapula—often in trauma.
- Sprains & Strains: Overstretching or tearing ligaments or muscle fibers.
- Adhesive Capsulitis (Frozen Shoulder): The joint capsule thickens and contracts, causing pain and loss of motion.
- The majority of chronic shoulder pain seen in clinical practice is related to rotator cuff pathology, impingement, and osteoarthritis.
Shoulder FAQs
1. What makes the shoulder the most flexible joint in the body?
The shallow ball-and-socket design paired with specialized muscle, ligament, and capsule structures allows movement in every direction—but also means less native bony stability.
2. What are the most common shoulder injuries?
Rotator cuff tears, impingement syndrome, dislocations, labral tears, fractures, and osteoarthritis are the greatest causes of pain and dysfunction.
3. How can I prevent shoulder injuries?
Maintain strong, balanced rotator cuff and scapular muscles, use correct technique during activities, avoid repetitive overhead movements, and address pain or stiffness early with mobility exercises.
4. What should I do after a shoulder injury?
Rest, ice, and see a specialist if motion is lost, pain is severe, or if there is deformity. Early assessment can guide the best path to safe recovery.
5. Are chronic shoulder injuries reversible?
Many are manageable with rehab, lifestyle changes, and appropriate conservative care. Some cases (such as severe arthritis or large tendon tears) may need procedural intervention, but most improve with proper therapy.
Take the First Step Toward Relief
Chronic shoulder pain does not have to control your life. The sooner evidence-based care begins, the faster recovery can start. Holistiq Health is committed to guiding you through every step—diagnosis, personalized treatment plan, insurance navigation, and psychological support.
Where Does It Hurt? We Can Help.