Dislocated Shoulder & Shoulder Instability
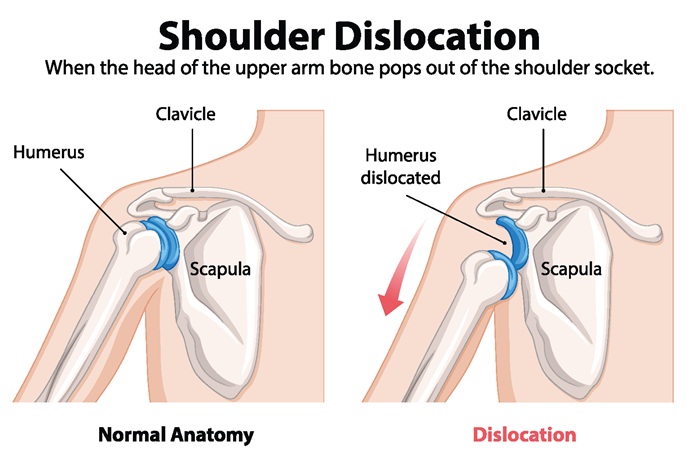
What Is a Dislocated Shoulder?
A shoulder dislocation occurs when the ball of the upper arm (humeral head) comes completely out of the socket on the shoulder blade (glenoid). Shoulder instability means the joint is loose or prone to slipping, with repeated subluxations (partial dislocations) or full dislocations. The shoulder is the most frequently dislocated major joint in the body, accounting for about 50% of all major joint dislocations.
Most traumatic dislocations are anterior (the ball moves forward), and a first‑time dislocation often injures stabilizing structures such as the labrum (Bankart lesion), capsule, and ligaments, which sets the stage for recurrent instability if not adequately rehabilitated.
Population‑based studies estimate the incidence of shoulder dislocation at around 24–25 per 100,000 person‑years in the United States and Europe, with a mean age in the mid‑30s and a strong peak in males aged 15–20 years. More than half of ED‑treated dislocations are sports‑related.
Who Is at Risk and Why It Happens
Common causes and risk factors include:
- Traumatic events: Falls, collisions, tackle sports, or accidents where the arm is forced outwards and backwards.
- Sports exposure: Basketball, football, rugby, wrestling, and overhead sports like volleyball, baseball, and swimming are frequent culprits.
- Structural tissue damage: Bankart lesions (labrum tears), capsular stretching, and bone loss on the glenoid or humeral head.
- Generalized laxity: People with naturally looser ligaments or connective tissue disorders may develop multidirectional instability even without major trauma.
Young age is a major predictor of recurrence. After a first traumatic anterior dislocation treated non‑operatively, recurrent instability rates range from 72–100% in patients under 20, 70–82% in those aged 20–30, and 14–22% in patients older than 50. In athletes aged 15–20 years, recurrence rates as high as 87% with non‑surgical management have been reported.
How Shoulder Instability Feels
Key symptoms include:
- Sudden severe pain and obvious deformity at the time of a true dislocation, with inability to move the arm until the shoulder is reduced.
- A feeling that the shoulder “slips out,” “gives way,” or is not secure, especially with the arm raised and rotated outward.
- Recurrent episodes of subluxation, catching, or clunking with certain motions.
- Apprehension or fear lifting the arm overhead or throwing.
- Weakness, fatigue, and reduced performance in sport or overhead tasks.
Red‑flag symptoms after injury—such as numbness, tingling, or weakness in the arm or hand—may indicate nerve or vascular involvement and warrant urgent assessment.
Meet Our Specialists

Trung Ha, MD

Raphael Ye, DO

Yasmin Fatemi, MD

Brian Lee, DC

Stephanie Yianitsas, PA-C

Diagnosis: From First Dislocation to Stability Plan
Evaluation typically involves:
- History: Mechanism of injury, number of dislocations, sports/work demands, age at first dislocation, and family or personal history of laxity.
- Physical exam:
- Inspection for deformity, atrophy, or scapular dyskinesis.
- Range of motion and strength testing.
- Specific instability tests (apprehension/relocation, load‑and‑shift, sulcus sign), performed carefully to avoid provoking full dislocation.
- Imaging:
- X‑rays to confirm reduction and identify fractures or bony Bankart/Hill‑Sachs lesions.
- MRI or MR arthrogram to assess the labrum, capsule, rotator cuff, and bone loss—critical for grading severity and selecting treatment.
Patients are often categorized as having traumatic unidirectional instability (common after sports injuries) or atraumatic/multidirectional instability (more common in generalized laxity), because patterns influence both prognosis and treatment choices.
Non‑Surgical Rehabilitation: The Foundation of Care
Acute phase after reduction:
- Short period in a sling for comfort (commonly 1–3 weeks), combined with early, pain‑free range of motion as guided.
- Swelling control and pain management to allow early participation in rehab.
Targeted physical therapy:
- Scapular stabilization and postural corrections to optimize shoulder mechanics.
- Progressive strengthening of the rotator cuff and periscapular muscles to keep the humeral head centered in the socket.
- Proprioceptive and neuromuscular training (closed‑chain drills, perturbation training) to improve joint awareness and dynamic stability.
- Sport‑ and job‑specific progressions to prepare for safe return to overhead work or contact sports.
Adjunctive care:
- Chiropractic and manual therapy to address cervical, thoracic, and rib motion that may influence shoulder loading.
- Anti‑inflammatory, strength‑supporting nutrition to aid recovery and maintain healthy body composition.
- Bracing or taping in certain sports or phases to provide external support while strength and coordination catch up.
Prospective data in in‑season athletes show that although 87% can return to play after initial non‑operative management, recurrent instability during the same season occurs in about 41%, and over half eventually opt for stabilization surgery in the off‑season. This underscores that rehab is essential but may not fully control recurrence risk in high‑demand, young populations.
Recurrence Risk: What the Numbers Say
Recurrent instability is the central challenge:
- Across all ages, approximately 20% of patients with an initial dislocation will experience one or more recurrent events; in many young cohorts, the proportion is much higher.
- Long‑term follow‑up of non‑operative management shows recurrence rates of about 72% in patients aged 12–22 years, 56% in those aged 23–29, and 27% in patients older than 30.
- Non‑operative treatment of first‑time anterior dislocation in young athletes yields recurrence rates ranging from 39–94% in prospective series.
Recurrent instability itself is associated with a higher risk of degenerative changes; one clinical summary notes that up to 40% of athletes with repeated instability episodes develop shoulder arthritis over time.
When Surgery Enters the Conversation
Because age, sport level, and instability pattern strongly influence recurrence risk, surgery is often considered in:
- Young (typically <25 years), highly active patients after a first traumatic dislocation.
- Individuals with recurrent dislocations despite a full, high‑quality rehab program.
- Patients with significant labral tears or bone loss documented on imaging.
Common procedures include:
- Arthroscopic Bankart repair and capsular plication to reattach the labrum and tighten the capsule.
- Bony augmentation procedures (e.g., Latarjet) in cases with substantial glenoid bone loss.
Systematic reviews and meta‑analyses in patients 15–25 years old show mean re‑dislocation rates of about 16% after operative stabilization versus 25% with non‑operative treatment, with better return‑to‑sport rates and patient‑reported outcomes in the surgical groups. In one classic randomized trial, recurrent instability at 2 years was 54% in conservatively treated patients but only 3% after open repair.
Even when surgery is chosen, pre‑ and post‑operative rehabilitation remain essential to restore strength, motion, and neuromuscular control and to optimize long‑term results.
Prognosis, Return to Sport, and Prevention
- For older or lower‑demand patients, many first‑time dislocations can be managed successfully with conservative care and do not necessarily require surgery.
- For adolescents and young adult athletes, the recurrence risk with non‑operative management is high—up to 72–100%—so a tailored plan that weighs sport goals against recurrence and arthritis risk is important.
- After surgical stabilization, most athletes can return to sport at similar levels, though contact and overhead athletes may require longer rehabilitation and careful progression.
Key prevention strategies include:
- Maintaining rotator cuff and scapular strength year‑round.
- Regular proprioceptive and stability drills, especially in overhead and contact athletes.
- Technique coaching and load management to avoid vulnerable positions (extreme abduction and external rotation under load).
- Early evaluation after any “slip” or subluxation episode rather than waiting for full dislocation.
FAQs
1. What is the difference between a shoulder dislocation and instability?
A dislocation happens when the ball of the shoulder completely comes out of the socket and usually requires reduction. Instability means the shoulder is loose or prone to slipping, with repeated partial or full dislocations over time.
2. How likely is my shoulder to dislocate again after a first injury?
Recurrence risk depends heavily on age and activity level. Younger athletes, especially under 25 and in contact or overhead sports, have a much higher chance of repeat dislocation than older or less active patients.
3. Can shoulder instability be treated without surgery?
Yes. Many patients improve with a structured non‑surgical program focusing on rotator cuff and scapular strengthening, neuromuscular control, posture, and sport‑specific retraining. Surgery is typically reserved for those with high recurrence risk or repeated dislocations despite good rehab.
4. When should I consider surgery for shoulder instability?
Surgery is often considered if you have recurrent dislocations, significant labral or bony injury on imaging, or you are a young, high‑demand athlete who wants to reduce the risk of future episodes after a first traumatic dislocation.
5. How long does rehab take, and when can I return to sports or heavy work?
Rehabilitation after a dislocation or stabilization procedure usually spans several months. Many people return to daily activities within weeks, but full return to contact or overhead sports often takes 4–6 months or more, depending on the severity of injury, treatment chosen, and adherence to the rehab plan.
Regain Your Shoulder’s Strength With Holistiq
Anyone who has felt a shoulder “pop out,” repeatedly slip, or never quite feel stable again should not wait for the next big injury. Early, expert assessment can clarify your true risk of recurrence and outline personalized options—from structured, non‑operative rehab to, when appropriate, modern stabilization procedures. Seeking care before instability becomes a chronic pattern offers the best chance to protect your shoulder, preserve performance, and avoid long‑term joint damage.
Where Does It Hurt? We Can Help.