Understanding Shoulder Arthritis
Causes and Impact of Shoulder Arthritis
Shoulder arthritis occurs when the smooth cartilage that cushions the shoulder joints wears down or becomes inflamed, leading to pain, stiffness, and loss of function. The two most common types affecting the shoulder are osteoarthritis (OA) and rheumatoid arthritis (RA). While OA is typically a “wear-and-tear” or post-injury condition, RA is an autoimmune disease that attacks the joint lining itself. Both can significantly impact daily life, but with the right plan, many people maintain excellent function without immediate surgery.

How Arthritis Changes Your Shoulder
The shoulder has two main joints:
- Glenohumeral joint – the ball-and-socket joint between the humeral head and the glenoid of the shoulder blade.
- Acromioclavicular (AC) joint – between the collarbone and the acromion at the top of the shoulder.
These joints are lined with cartilage and surrounded by synovial tissue (the joint lining) that produces lubricating fluid. In arthritis:
- Cartilage thins and breaks down.
- Bone may form spurs (osteophytes).
- Synovial tissue becomes inflamed and thickened (especially in RA).
- The joint space narrows, causing grinding, stiffness, and pain.
Over time, this can alter shoulder mechanics and overload nearby structures like the rotator cuff, bursae, and surrounding muscles.
Osteoarthritis vs Rheumatoid Arthritis in the Shoulder
Shoulder Osteoarthritis (OA)
Osteoarthritis is primarily degenerative:
- Often develops with age or after prior injuries (fractures, dislocations, rotator cuff tears).
- May involve the glenohumeral joint, the AC joint, or both.
- Cartilage gradually wears away, exposing bone.
- Common in people with physically demanding jobs, heavy lifting histories, or previous shoulder surgery.
Shoulder Rheumatoid Arthritis (RA)
Rheumatoid arthritis is an autoimmune disease:
- The immune system attacks the synovial lining of joints, including the shoulders.
- Leads to chronic inflammation, pain, cartilage damage, and bone erosion.
- Often affects multiple joints symmetrically (both shoulders, hands, wrists, knees).
- May be associated with fatigue, low-grade fevers, and other systemic symptoms.
Other inflammatory conditions (psoriatic arthritis, gout, CPPD) can also affect the shoulder but are less common. Your plan may reference them briefly for context.
Who Is at Risk?
Osteoarthritis – higher risk if you:
- Are over age 50.
- Have a history of shoulder trauma, dislocation, or surgery.
- Perform repetitive overhead or heavy work.
- Have long-standing rotator cuff tears.
- Are overweight or have other load-related joint problems.
- Have a family history of osteoarthritis.
Rheumatoid Arthritis – higher risk if you:
- Have a personal or family history of autoimmune disease.
- Are female (RA is more common in women).
- Are a current or former smoker.
- Have other autoimmune conditions or systemic inflammatory issues.
Both OA and RA can coexist with shoulder bursitis, impingement, or rotator cuff disease, which can make symptoms more intense and complex.
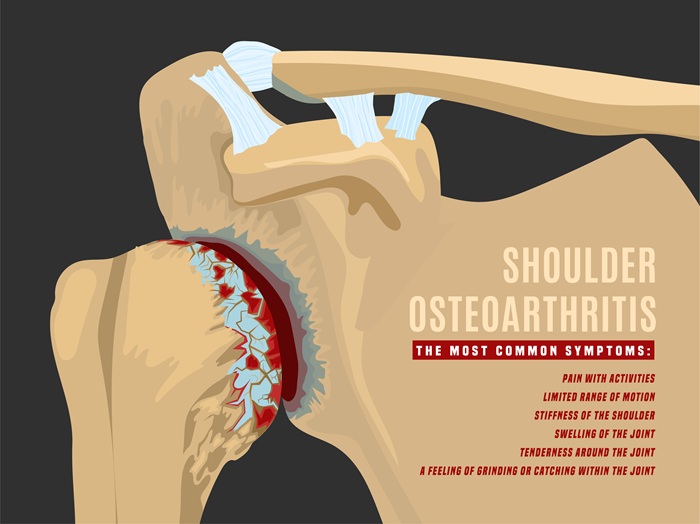
Common Symptoms of Shoulder Arthritis
Patients with shoulder arthritis frequently report:
- Deep, ache-like pain in the joint, often worse with use.
- Stiffness and reduced range of motion, especially raising the arm or reaching behind the back.
- Grinding, popping, or “crepitus” as the joint moves.
- Weakness and difficulty performing daily tasks (dressing, lifting, grooming, reaching overhead).
- Night pain, often disturbing sleep when lying on the affected side.
Differences between OA and RA symptoms:
- OA – Pain typically worsens with activity and improves with rest; stiffness may be brief in the morning.
- RA – Longer-lasting morning stiffness, swelling, and “warm” joints; often accompanied by fatigue and pain in other joints.
Red flag symptoms that need urgent attention:
- Sudden severe pain and swelling.
- Red, hot joint with fever (possible infection).
- Rapid loss of function or inability to move the arm.
Meet Our Specialists

Trung Ha, MD

Raphael Ye, DO

Yasmin Fatemi, MD

Brian Lee, DC

Stephanie Yianitsas, PA-C

How Shoulder Arthritis Is Diagnosed
A comprehensive evaluation includes:
1. History and Physical Exam
- Onset and duration of pain.
- Prior injuries or surgeries.
- Activity level, work demands, and medical history.
- Physical exam looks at:
- Active and passive range of motion.
- Strength of the rotator cuff and surrounding muscles.
- Crepitus (grinding) and deformity.
- Tenderness over specific joints (glenohumeral vs AC).
2. Imaging
- X-rays – Show joint space narrowing, bone spurs, cysts, and bone changes typical of OA and advanced RA.
- Ultrasound – Useful to evaluate rotator cuff, bursae, and soft tissues when arthritis coexists with tendon or bursal problems.
- MRI or CT – Used when more detail is needed (complex cases, surgical planning, suspicion of additional pathology).
3. Laboratory Testing (especially when RA is suspected):
- Rheumatoid factor (RF).
Anti-CCP antibodies. - Inflammatory markers (ESR, CRP).
- Other autoimmune or metabolic panels when indicated.
These findings help distinguish arthritis from frozen shoulder, isolated rotator cuff tears, impingement, or isolated bursitis.
Holistiq’s Non-Surgical Shoulder Arthritis Care Plan
1. Education and Expectations
- Clearly explain the type of arthritis and stage of disease.
- Set realistic goals: symptom control, functional improvement, and slowing progression.
- Reinforce that arthritis is often manageable long-term with the right plan.
2. Anti-Inflammatory Nutrition & Metabolic Support
- Personalized nutrition strategies focusing on:
- Whole, minimally processed foods.
- Anti-inflammatory ingredients (omega-3 rich fish, olive oil, nuts, seeds, colorful vegetables and fruits).
- Reduced refined sugars and processed fats.
- Weight management to reduce joint load.
- Coordination with diabetes or metabolic care when needed.
- For RA, collaboration with rheumatology to optimize systemic therapy (DMARDs, biologics) while supporting overall health.
3. Physical Therapy: Mobility, Strength, and Protection
- Range-of-motion work to prevent further stiffness and maintain functional arcs of movement.
- Strengthening exercises for rotator cuff and scapular stabilizers to:
Improve joint mechanics.
Reduce stress on arthritic surfaces. - Postural retraining to optimize alignment and shoulder loading.
- Joint protection techniques:
- Proper lifting and reaching strategies.
- Activity pacing to prevent flares.
- Tailored home exercise plans to maintain improvements between sessions.
4. Chiropractic Care and Manual Therapy
- Gentle joint mobilizations to improve movement, especially in early to moderate stages.
- Soft tissue therapy to ease muscle tension and compensatory tightness.
- Work on the neck, upper back, and rib cage to normalize mechanics and reduce shoulder overload.
5. Shockwave and Adjunctive Modalities (As Appropriate)
- Shockwave may be considered for associated tendinopathies (such as rotator cuff involvement) or chronic soft tissue pain around the arthritic joint.
- Other modalities may include heat, ice, therapeutic ultrasound, and electrical stimulation to manage pain and improve tolerance for exercise.
6. Injections and Interventional Pain Management
- Corticosteroid injections into the glenohumeral or AC joint to:
- Reduce inflammation.
- Provide short- to medium-term pain relief.
- Create a window for more effective rehab.
- Other injection options may be considered based on severity and evidence, such as viscosupplementation in selected cases.
- Injections are used judiciously and always paired with lifestyle and rehab interventions.
7. Regenerative Medicine for Osteoarthritis
- Platelet-rich plasma (PRP) and other biologic approaches can be considered for early-to-moderate osteoarthritis:
- Aims to reduce pain and improve function over the longer term.
- Often used as an adjunct when standard conservative measures are not sufficient.
Not typically first-line for RA, where systemic immune control is primary, but may play a supportive role for specific OA components.
When Surgery Becomes an Option
Non-surgical care remains the focus as long as it provides meaningful relief and function. Surgery may be discussed when:
- Pain is severe and constant despite optimized conservative treatment.
- Stiffness and weakness significantly impair daily activities (dressing, working, sleeping).
- Imaging shows advanced, end-stage joint destruction.
Surgical options, typically performed by orthopedic surgeons, may include:
- Total shoulder arthroplasty (replacement) – replacing both sides of the joint.
- Reverse shoulder arthroplasty – used when there is severe arthritis and large rotator cuff tears.
- Hemiarthroplasty – replacing only part of the joint in select cases.
Even when surgery is needed, preoperative conditioning and postoperative rehab—integrated with holistic care—are critical to achieving the best results.

Living Well with Shoulder Arthritis
What to Expect During Recovery
Although arthritis is chronic, many people maintain active, fulfilling lives with the right strategies:
- Stay consistent with home exercise and stretching routines.
- Maintain a healthy weight and balanced diet.
Adapt work and daily activities to reduce strain without stopping movement altogether. - Plan for rest periods and pacing to avoid flares.
- Maintain regular check-ins to adjust your treatment plan as needs change.
For RA, strict adherence to disease-modifying therapy and regular monitoring are essential to protect not just the shoulders but all affected joints and organ systems.
Frequently Asked Questions
Is shoulder arthritis reversible?
Arthritic changes to cartilage and bone are generally not reversible, but symptoms can be significantly reduced, and function can be improved with comprehensive care. The goal is to slow or halt progression and keep you active.
How do I know if my pain is from arthritis or from a rotator cuff tear?
Arthritis tends to cause deep joint pain, stiffness, and grinding, especially with movement and over time. Rotator cuff tears often produce weakness and pain with specific movements and may not always cause grinding. A thorough exam and imaging help distinguish between them—and both can occur together.
Can I avoid shoulder replacement with conservative treatment?
Many patients do. For mild to moderate arthritis, non-surgical care often provides long-term relief. Even in more advanced cases, conservative care can delay surgery and optimize your condition if surgery is eventually needed.
What’s different about RA in the shoulder compared to osteoarthritis?
RA is immune-driven, often affects both shoulders, and is associated with whole-body symptoms and other joint involvement. Osteoarthritis is more localized, degenerative, and often linked to age or prior injury. Treatment for RA always includes systemic immune management.
Will exercise make my arthritis worse?
Appropriate exercise is protective, not harmful. High-impact or poorly designed programs can aggravate symptoms, but guided therapy and tailored exercise improve joint health and reduce pain.
Does Holistiq accept my insurance for arthritis treatment?
Holistiq Health accepts major health insurance plans and can assist with verifying coverage and estimating out-of-pocket costs.
Take Control of Your Shoulder Pain
If shoulder pain, stiffness, or arthritis has started to limit your daily life, you don’t have to wait for it to get worse. Holistiq Health offers an integrated, conservative shoulder arthritis program that blends anti-inflammatory nutrition, physical therapy, chiropractic care, advanced modalities, regenerative options, and targeted injections—coordinated with rheumatology and primary care when needed.
Where Does It Hurt? We Can Help.