Calcific Tendonitis
When Calcium Crystals Invade the Rotator Cuff
Calcific tendonitis is a condition where calcium deposits form inside a tendon, most often in the rotator cuff of the shoulder (especially the supraspinatus tendon). These deposits can increase pressure within the tendon and irritate surrounding structures, leading to inflammation, pain, and stiffness. Unlike standard tendonitis, calcific tendonitis specifically involves visible calcium buildup, which usually shows up clearly on X‑ray or ultrasound.
Epidemiological studies suggest that calcific deposits in the rotator cuff are present in about 2.5–7.5% of healthy adult shoulders, even when people have no symptoms. Among patients who present with shoulder pain, calcific tendonitis is responsible for about 10–42% of chronic painful shoulders, and some series estimate that 10–20% of shoulder pain diagnoses in specialty clinics are due to calcific tendonitis.
Calcific tendonitis typically progresses through three overlapping phases:
- Formative phase: Calcium begins to accumulate inside the tendon, sometimes with mild or no symptoms.
- Resting phase: The deposit is relatively stable; pain may be intermittent or minimal.
- Resorptive phase: The body attempts to break down and reabsorb the deposit, causing intense local inflammation and often severe pain.

Why Do These Calcium Deposits Form?
The exact cause remains unclear, but calcific tendonitis is thought to be a cell‑mediated, reactive process rather than simple “wear and tear.” Mechanical overload, microtrauma, and altered blood supply all may trigger abnormal tendon healing and calcium deposition.
Recognized risk factors include:
- Age 30–60 years, with a clear peak in the fourth and fifth decades of life
- Higher frequency in women, who account for roughly 70% of cases in some series
- Repetitive overhead activity or prior tendon irritation, although large studies suggest calcific tendonitis is not always strongly linked to physical activity level
- Possible associations with endocrine or metabolic disorders such as diabetes and thyroid disease
A large cohort study found calcific deposits in 7.8% of asymptomatic adults and in 42.5% of patients with subacromial pain syndrome, confirming that deposits are common but become symptomatic in a subset of people. Bilateral deposits occur in roughly 10–20% of patients.
The Pain Experience: How Calcific Tendonitis Shows Up
Calcific tendonitis can range from a nagging ache to sudden, severe pain. Typical symptoms include:
- Sharp or burning pain in the outer shoulder, often worsening when lifting the arm or reaching overhead
- Marked difficulty sleeping on the affected side, particularly during the resorptive phase
- Painful and limited range of motion from muscle guarding
- Night pain, which may be intense and throbbing
- Occasional swelling or a sense of fullness in the shoulder
Acute flares can be so painful that they are mistaken for fractures, frozen shoulder, or major rotator cuff tears. Long‑standing or milder cases may feel more like stubborn rotator cuff tendinopathy.
Calcific tendonitis can coexist with rotator cuff tears, although modern imaging studies suggest this happens in a minority of cases: roughly 15–28% in large MRI and ultrasound series, with most of those tears being partial thickness.
Meet Our Specialists

Trung Ha, MD

Raphael Ye, DO

Yasmin Fatemi, MD

Brian Lee, DC

Stephanie Yianitsas, PA-C

Pinpointing the Problem: How Diagnosis Is Made
Diagnosis relies on a combination of clinical assessment and imaging.
Clinical Story and Hands‑On Exam
A clinician will review:
- When symptoms started and how they have progressed
- What activities aggravate or relieve pain
- Any prior shoulder injuries or conditions
Physical exam typically includes:
- Assessing active and passive shoulder range of motion
- Testing rotator cuff strength
- Identifying a “painful arc” with mid‑range arm elevation
- Palpating tender points along the rotator cuff and bursa
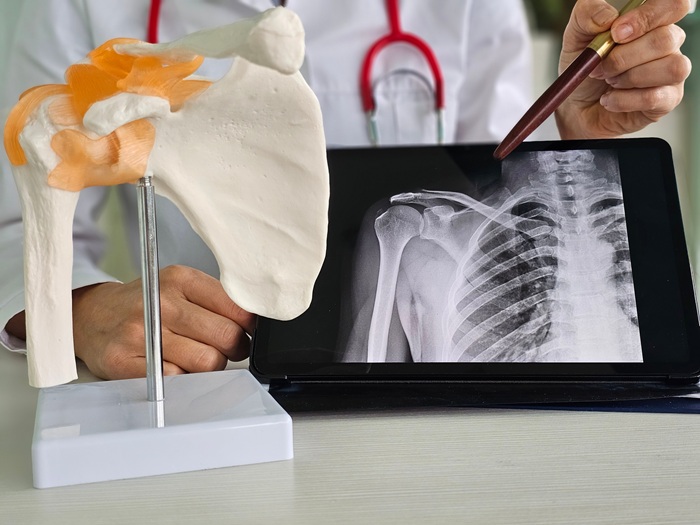
Imaging the Calcium: X‑ray, Ultrasound, MRI
Imaging is crucial to confirming calcific tendonitis and evaluating associated problems:
- X‑rays: Show dense, cloud‑like or well‑defined white deposits within or adjacent to the rotator cuff tendons.
- Ultrasound: Characterizes deposit size, shape, and consistency and guides injections or lavage procedures.
- MRI: Used when additional pathologies (rotator cuff tears, bursitis, labral injury) are suspected or when planning more advanced interventions.
Reported incidence rates of rotator cuff calcific tendinopathy range from about 6.8% to 54% depending on population and imaging criteria, highlighting how frequently these deposits are identified when the shoulder is imaged.
Holistiq’s Whole‑Person Blueprint for Non‑Surgical Care
Early Pain and Activity Management
In the painful resorptive phase, the priority is rapid symptom control without completely immobilizing the joint:
- Temporary avoidance of heavy or overhead activities
- Gentle, pain‑limited movement to prevent secondary stiffness
- Ice or alternating ice and heat to reduce pain and swelling
- Short‑term use of anti‑inflammatory or analgesic medications when appropriate
Clear instructions on what to pause and what to continue help minimize disability while avoiding further irritation.
Anti‑Inflammatory Nutrition
Systemic inflammation can amplify local tendon pain. An anti‑inflammatory diet supports the body’s capacity to heal:
- Emphasizing vegetables, fruits, whole grains, legumes, and lean protein
- Including healthy fats such as omega‑3 rich fish, nuts, seeds, and olive oil
- Reducing refined sugars, ultra‑processed foods, and trans fats
Addressing underlying metabolic issues, such as diabetes or thyroid dysfunction, may also help reduce recurrence risk and support overall tendon health.
Targeted Physical Therapy
Once pain is somewhat controlled, guided rehabilitation becomes the backbone of recovery:
- Range‑of‑motion work: Gentle, progressive stretching to restore elevation and rotation without provoking flares.
- Strengthening: Focus on rotator cuff and scapular stabilizers to normalize shoulder mechanics and reduce load on the affected tendon.
- Posture and movement retraining: Correcting rounded shoulders, forward head posture, and faulty lifting or reaching patterns.
- Gradual return‑to‑activity: A staged plan to safely reintroduce work, sport, and fitness tasks.
Targeted exercise is crucial to convert improvements in pain and structure into lasting functional gains.
Chiropractic and Manual Care
Chiropractic care and manual techniques can enhance recovery:
- Joint mobilizations to improve glenohumeral and scapulothoracic motion
- Soft‑tissue and myofascial release for tight or overworked muscles
- Addressing related restrictions in the cervical and thoracic spine that may contribute to overload of the shoulder
These hands‑on methods are typically integrated with an active rehab program rather than used in isolation.
Shockwave Therapy
Extracorporeal shockwave therapy (ESWT) is a key non‑surgical option in chronic calcific tendonitis:
- High‑energy acoustic waves are delivered to the area of the deposit from outside the body.
- Shockwave can fragment calcific deposits, stimulate blood flow, and promote tendon healing.
- Multiple randomized trials and systematic reviews show that high‑energy ESWT significantly improves pain, function, and calcification resolution compared with placebo or low‑energy treatment.
- In one prospective trial of 195 patients with chronic calcific tendonitis, high‑energy ESWT produced pain relief in up to 58% of patients versus 5% in the control group, with dose‑dependent improvements in function and radiologic disintegration of deposits at six months.
- A JAMA trial reported complete disappearance of calcific deposits in 60% of patients at six months and 86% at twelve months after high‑energy ESWT, compared with 11–25% in the sham group.
ESWT is usually performed in a series of outpatient sessions and combined with a strengthening and mobility program for best outcomes.
Injections and Interventional Pain Management
If symptoms remain intense or refractory:
Corticosteroid injections:
- Can rapidly reduce inflammation around the deposit and in the subacromial bursa.
- Often used to create a window for more effective participation in physical therapy.
These options are reserved for selected cases and are always deployed within a broader rehabilitation and prevention strategy.
Regenerative Options
In chronic or recurrent calcific tendonitis with residual tendon degeneration after the main calcific phase, regenerative approaches may be considered:
- Platelet‑rich plasma (PRP) injections aim to enhance tendon healing and remodeling.
- Evidence is still evolving, and PRP is generally considered after conventional conservative measures and, when appropriate, shockwave or lavage.
The suitability of regenerative therapies depends on the patient’s overall status, imaging findings, and response to prior treatments.
Recovery Trajectory
The natural history of calcific tendonitis is often favorable, especially when guided by appropriate care:
- Population studies indicate that many patients achieve good or excellent function in the long term, though a subset continues to report some residual symptoms years later.
- Acute flares can settle dramatically within days to weeks with proper management.
- Functional recovery typically occurs over several weeks to a few months of consistent rehab.
- Radiographic remodeling of deposits may take months to years, but clinical improvement often precedes complete radiologic resolution.
A large long‑term study of rotator cuff calcific tendinopathy reported that after an average of fourteen years, most patients achieved acceptable function, though about 42% still had some degree of functional limitation, underscoring the importance of early, structured care and ongoing shoulder conditioning.

Keeping Calcium Away: Long‑Term Shoulder Protection Strategies
To reduce the chance of recurrent calcific tendonitis or related shoulder issues:
- Maintain regular shoulder flexibility and strengthening exercises even after pain resolves.
- Avoid abrupt increases in overhead or high‑load activities; build volume and intensity gradually.
- Pay attention to posture at work and during daily tasks, especially if you sit or lift frequently.
- Warm up thoroughly before exercise and use proper technique in sports and resistance training.
- Work with your care team to monitor and manage metabolic or endocrine conditions that may contribute to tendon problems.
Calcific Tendonitis FAQ
How common is calcific tendonitis?
Calcific deposits in the rotator cuff are seen in roughly 2.5–7.5% of healthy adult shoulders, and in some series, calcific tendonitis accounts for 10–42% of chronic painful shoulders.
Can calcific tendonitis resolve on its own?
Yes. Many deposits partially or completely resorb over time, especially during the resorptive phase, and spontaneous resolution has been documented in imaging follow‑ups. However, symptoms during that process can be severe, and structured care often makes the course shorter and more tolerable.
Do all calcium deposits need to be removed?
No. Treatment focuses on pain and function, not just the presence of a deposit. In many cases, deposits can remain or slowly shrink without surgery if symptoms are well controlled.
How effective is shockwave therapy?
High‑energy ESWT has been shown in randomized trials to significantly improve pain and function and to accelerate calcification resolution compared with placebo or lower energy doses, with complete disappearance of deposits in up to 60–86% of patients at six to twelve months in some studies.
Is surgery always necessary if conservative treatments fail?
Not always, but surgery is considered when pain and functional limitations remain significant despite a full course of conservative care, including ESWT and, when appropriate, lavage. Arthroscopic removal of the deposit and treatment of coexisting issues can produce good outcomes, but both operative and nonoperative approaches are likely to yield clinically meaningful improvements in most chronic cases.
Does insurance cover treatment for calcific tendonitis?
Most standard evaluations, imaging, physical therapy, chiropractic care, and injections are covered by major health insurance plans, though coverage for ESWT or regenerative procedures varies by policy. Clinics can help patients verify specific benefits and out‑of‑pocket costs.
Take Control of Your Shoulder Pain
Take the next step toward lasting shoulder relief. Schedule a comprehensive evaluation today to find out what’s causing your pain and get a customized, conservative treatment plan that fits your life. Early, holistic care can help you avoid unnecessary surgery, restore confidence in your movement, and get you back to the activities you love.
Where Does It Hurt? We Can Help.