Middle Back Pain Overview
Thoracic Back Pain at a Glance
Middle back pain is common, often posture‑related, but can sometimes signal more serious spine or organ problems. This overview explains what “middle back” pain is, why it happens, how it is diagnosed and treated, and when to seek help—supported by key statistics so patients understand their risks and options.
Why Middle Back Pain Deserves Attention
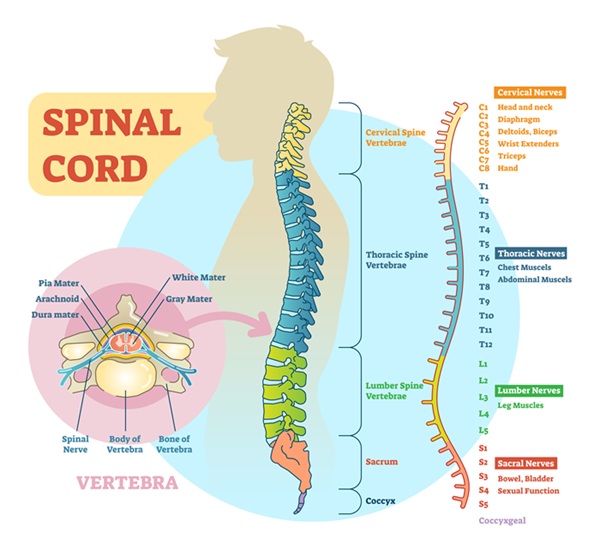
Middle back pain refers to pain in the thoracic spine—the area between the base of the neck and the bottom of the rib cage, often felt “between the shoulder blades” or around the bra‑line region. The thoracic spine includes 12 vertebrae (T1–T12) and the ribs, linking the neck, chest, and low back.
Population studies show thoracic spine pain is less common than neck or low‑back pain but still significant, with point prevalence estimates ranging from about 4% to over 13% of adults and lifetime prevalence around 16–20% depending on definitions and age. One occupational study reported that 1 in 10 men and 1 in 5 women in a working population experienced thoracic spine pain.

Why the Middle Back Hurts
Middle back pain can come from muscles, joints, discs, nerves, ribs, or even organs that refer pain into the area.
Common Musculoskeletal Causes
- Muscle strain and poor posture
- Long periods of sitting, slouching, or “hunched over” work (computers, phones, driving) overload the mid‑back muscles and ligaments.
- Repetitive lifting, twisting, or overhead work can strain the paraspinal and scapular muscles.
- Facet joint and disc degeneration
- Like other parts of the spine, thoracic facet joints and discs can develop age‑related wear, causing aching or sharp pain with movement.
- Thoracic disc herniation is rare—estimated at only 0.25–1% of all disc herniations—but can cause mid‑back pain with band‑like chest/rib symptoms or neurologic changes.
- Rib and costovertebral joint dysfunction
- Irritation where the ribs meet the spine or sternum can cause sharp, localized pain that may worsen with deep breaths, coughing, or rotation.
- Postural deformities (kyphosis, scoliosis)
- Excessive rounding of the upper back or sideways curvature can increase mechanical stress and muscular fatigue in the mid‑back.
Referred and Serious Causes
- Referred pain from neck or shoulders – cervical or shoulder problems can create pain between the shoulder blades.
- Visceral and serious pathology – although less common, mid‑back pain can reflect:
- Cardiac issues, aortic problems, or lung disease
- Gallbladder, stomach, or other abdominal organ disease
- Osteoporotic vertebral fracture, infection, or tumor
A large review found thoracic spine pain is often associated with other musculoskeletal pain, backpack or posture factors, and mental health, especially in adolescents.
Typical Middle Back Pain Symptoms
- Aching, burning, or tightness between the shoulder blades or along the mid‑spine
- Stiffness, especially after sitting or first thing in the morning
- Sharp or catching pain with certain movements, deep breathing, or twisting
- Pain that improves with gentle movement and worsens with prolonged sitting or slouching
If thoracic nerves or the spinal cord are involved, symptoms may include:
- Band‑like pain or altered sensation around the chest or abdomen
- Numbness, tingling, or weakness in the trunk or legs
- Balance problems or gait changes

Mid Back Pain Evaluation
Most patients start with a careful history and physical exam, with imaging reserved for cases where it will change management.
History and Physical Exam
History
- Onset (sudden vs gradual), location, radiation
- Work and activity patterns (desk work, lifting, sports)
- Posture, previous spine problems, and other joint pain
- Systemic symptoms (fever, weight loss, shortness of breath, GI symptoms)
Physical exam
- Posture and spine alignment (kyphosis, scoliosis)
- Range of motion and pain with flexion, extension, rotation
- Palpation over joints, muscles, and ribs for tenderness or spasm
- Neurologic exam (sensation, strength, reflexes) if nerve or cord involvement is suspected
Imaging and Tests
- X‑rays – to evaluate fractures, alignment, and significant degenerative changes.
- MRI – for suspected disc herniation, spinal cord compression, infection, or tumor.
- CT or bone scan – in select cases (e.g., subtle fractures or complex anatomy).
- Lab tests – if infection, inflammatory disease, or malignancy is suspected.
Thoracic disc herniations are rare (0.1–5% of all reported disc herniations, affecting roughly 1 in 1,000 to 1 in 1,000,000 people), but MRI is key when symptoms suggest this diagnosis.
Treatment Options for Middle Back Pain
Most mechanical middle back pain responds well to conservative care focused on movement, posture, and strengthening.
Conservative In‑Clinic Care
- Manual therapy and chiropractic care
- Gentle mobilization or adjustment of thoracic spine and ribs to restore movement and reduce pain.
- Soft‑tissue techniques and myofascial release to address tight or overworked muscles.
- Physical therapy and rehabilitation
- Thoracic mobility exercises and stretches
- Scapular and upper‑back strengthening
- Core stability and breathing mechanics training
- Personalized programs for desk workers, manual labor, or athletes
- Pain‑relief strategies
- Short‑term use of NSAIDs or other medications as appropriate (coordinated with a physician).
- Targeted injections (e.g., trigger point injections, facet or costovertebral joint injections) when indicated by examination and imaging.
Lifestyle, Posture, and Ergonomics
- Workstation setup to reduce slouching and forward‑head posture
- Regular posture “resets” and movement breaks during desk work
- Education on lifting mechanics, sport technique, and daily activity habits
Longitudinal data suggest thoracic spine pain often coexists with other spinal pain and can become recurrent without addressing posture, ergonomics, and general health.
Home Strategies to Support Healing
Safe, general strategies can help many patients with non‑serious middle back pain.
Gentle Movement and Mobility
- Thoracic extension over a towel or foam roll (within comfort)
- Cat‑camel or similar spinal mobility drills
- Shoulder blade squeezes and wall slides to strengthen postural muscles
If any exercise causes sharp pain, radiating symptoms, shortness of breath, or chest pain, stop and seek evaluation.
Heat, Ice, and Activity Pacing
- Ice may help after acute strain or injury.
- Heat often helps chronic muscular tightness and stiffness.
- Gradual return to activity, avoiding both prolonged bed rest and sudden intense workouts.
Posture and Daily Habits
- Alternate sitting and standing; avoid staying in one posture for long.
- Keep screens at eye level, with shoulders relaxed and back supported.
- Choose a mattress and pillow combination that supports neutral spine alignment to reduce night‑time mid‑back strain.

When to See a Specialist
Consider a professional evaluation if:
- Middle back pain lasts more than 4–6 weeks despite home care
- Pain recurs frequently or is gradually worsening
- Pain interferes with sleep, work, or daily activities
- You notice arm, chest, or trunk numbness, tingling, or weakness
- You are unsure whether your symptoms could be coming from the heart, lungs, or abdominal organs
A spine‑focused clinic can:
- Confirm whether pain is mechanical, nerve‑related, or referred from elsewhere
- Create an integrated care plan (manual therapy, rehab, injections where appropriate, and lifestyle coaching)
- Coordinate with primary care, cardiology, or other specialists if red‑flags or systemic conditions are suspected.
FAQs: Middle Back Pain
What are the most common causes of pain between the shoulder blades?
The most frequent causes include muscle strain from poor posture or overuse, joint and disc wear in the thoracic spine, rib or costovertebral joint irritation, and referred pain from the neck or shoulders. Less commonly, heart, lung, or abdominal problems can cause similar discomfort.
Do I need an MRI if I have middle back pain?
Not usually. Many cases can be diagnosed with history and physical exam. MRI is typically reserved for people with red‑flag symptoms, significant neurologic findings, suspicion of serious pathology, or persistent pain not responding to appropriate conservative treatment.
How rare is a thoracic disc herniation?
Thoracic disc herniations are uncommon, estimated to represent about 0.25–1% of all disc herniations, and overall reported rates in the literature range from 0.1–5% depending on the series. They can mimic cardiac, abdominal, or other conditions, so accurate diagnosis often requires MRI and specialist evaluation.
Can poor posture really cause long‑term middle back pain?
Yes. Studies show thoracic spine pain is associated with postural factors, backpack use, and occupational demands, especially in younger people. Chronic slouching or prolonged sitting increases load on the thoracic spine and surrounding muscles, contributing to persistent mid‑back ache and tightness.
When should I be worried that mid‑back pain is from my heart or lungs?
Seek urgent care if mid‑back pain occurs with chest pain, shortness of breath, jaw or arm pain, sudden onset with exertion, or if you feel acutely unwell—these can signal cardiac, aortic, or pulmonary problems. Persistent mid‑back pain with cough, weight loss, or night sweats also warrants prompt medical review.
Will my middle back pain go away on its own?
Many posture‑ or muscle‑related cases improve over days to weeks with movement, ergonomic changes, and conservative care. However, thoracic spine pain can become recurrent or chronic, and is often linked to other spinal pain and lifestyle factors, so early attention to posture, strength, and health habits improves long‑term outcomes.
Regain Your Neck Strength With Holistiq
Neck pain can be frustrating and draining, but it is rarely something you have to live with permanently. A mix of smart home care, ergonomic changes, and targeted conservative treatments (like chiropractic, physical therapy, and, when needed, injections) can dramatically reduce pain and improve function for most people. If your pain isn’t improving or you’re not sure what is safe to do, an expert evaluation is the safest first step toward lasting, confident relief.
Where Does It Hurt? We Can Help.