Hip Pain Causes, Symptoms & Non‑Surgical Treatment
Hip Pain
- Hip Pain Overview
- Avascular Necrosis
- Bursitis
- Gluteal Tendinopathy
- Pain by Activity (Walking, Running, Sitting, Sleeping)
- Pain in Athletes
- Pain in Older Adults
- Pain by Location (Front, Side, Rear)
- Iliopsoas Pain
- Impingement Syndrome
- Labral Tear
- Osteoarthritis
- Pain After Hip Replacement
- Piriformis Syndrome
- Snapping Hip Syndrome
How Common Is Hip Pain?
Hip pain is common and can significantly limit walking, exercise, work, and sleep, but many causes are treatable without surgery when identified early. This guide explains major causes, key symptoms, and the main non‑surgical options available.
- In the general adult population, about 1 in 10 people report hip pain, and prevalence increases with age.
- In one large survey, 14.3% of adults reported significant hip pain on most days over a 6‑week period.
- Chronic hip pain is strongly associated with difficulty in basic activities such as standing up, walking, and climbing stairs, leading to reduced quality of life.
What Are the Most Common Causes of Hip Pain?
1. Hip Osteoarthritis and Other Arthritis
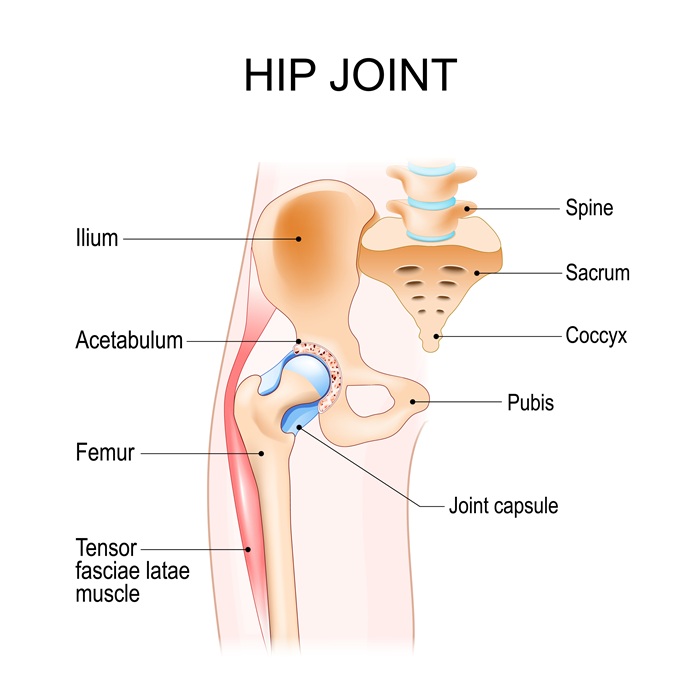
Degenerative osteoarthritis is the leading chronic cause of hip pain in middle‑aged and older adults, resulting from cartilage breakdown and joint inflammation. Rheumatoid and other inflammatory arthritides can also affect the hip. Patients typically notice deep aching pain, stiffness after rest, and gradual loss of motion.
2. Hip Labral Tears and Femoroacetabular Impingement (FAI)
In younger and active adults, structural abnormalities of the ball‑and‑socket joint (FAI) and labral tears are common sources of groin‑predominant hip pain. People often describe sharp pain with twisting, squatting, prolonged sitting, or pivoting, sometimes with catching or clicking.
3. Bursitis and Lateral Hip Pain
Trochanteric bursitis and related conditions such as greater trochanteric pain syndrome cause aching or sharp pain over the outer hip, often worse when lying on that side or climbing stairs. Repetitive friction, overuse, trauma, or underlying tendon problems can inflame the bursa.
4. Tendon and Muscle Problems
Gluteal tendinopathy, hip flexor strain, hamstring strain, and adductor (groin) strain can all produce hip‑region pain, particularly after sports, sudden overexertion, or new activities. Symptoms often include localized tenderness, pain with specific movements, and sometimes weakness or limping.
5. Bone and Structural Disorders
Conditions such as hip fractures, especially in older adults with osteoporosis, and avascular necrosis (loss of blood supply to the femoral head) can cause severe hip pain and disability. These often present with sudden or escalating pain and difficulty bearing weight.
6. Referred Pain from Spine and Sacroiliac Joint
The hip region may hurt even when the primary problem is in the lumbar spine, sacroiliac joint, or nerves (e.g., sciatica). In such cases, pain may radiate from the back or buttock into the hip, often with numbness, tingling, or weakness.
Meet Our Specialists

Trung Ha, MD

Raphael Ye, DO

Yasmin Fatemi, MD

Brian Lee, DC

Stephanie Yianitsas, PA-C

What Symptoms Help Identify the Source of Hip Pain?
Pain Location
- Groin/anterior hip: often suggests intra‑articular problems such as osteoarthritis, FAI, or labral tear.
- Outer/lateral hip: more often bursitis or gluteal tendinopathy.
- Buttock/posterior hip: may indicate spine, sacroiliac joint, piriformis syndrome, or hamstring issues.
Pain Pattern and Activity Triggers
- Pain with walking/standing: common in arthritis, tendinopathy, bursitis, and stress fractures.
- Pain with sitting or deep flexion: frequently associated with FAI and labral pathology.
- Night pain/lying on side: typical of lateral bursitis or advanced arthritis. or rotation.
Red‑Flag Symptoms Requiring Urgent Evaluation
- Sudden, severe hip pain after a fall or trauma.
- Inability to bear weight on the affected leg.
- Hip pain with fever, chills, or redness/warmth over the joint (possible infection).
- History of cancer, unexplained weight loss, or night‑dominant pain.
A large review found thoracic spine pain is often associated with other musculoskeletal pain, backpack or posture factors, and mental health, especially in adolescents.

How Is Hip Pain Diagnosed?
Clinical Evaluation
A careful history and physical exam provide the foundation for diagnosis. Clinicians ask about location, onset, radiation, injury, medical conditions, and what makes pain better or worse. Physical tests evaluate range of motion, strength, gait, and specific maneuvers such as impingement tests, FABER, single‑leg stance, and palpation over bursae or tendons to localize the source.
Imaging
- X‑rays: typically the first test, used to identify arthritis, fractures, alignment issues, or bone deformities.
- MRI/MR arthrogram: provides detailed images of cartilage, labrum, tendons, and early avascular necrosis, and is often used for persistent or complex cases.
- Ultrasound: useful for diagnosing bursitis, tendon pathology, and guiding injections.
Neurodiagnostic Testing
Electromyography (EMG) and nerve conduction studies may be used when there is suspicion of nerve root compression or peripheral nerve entrapment, such as sciatica or meralgia paresthetica.
What Non‑Surgical Treatments Are Available for Hip Pain?
Activity Modification and Lifestyle Changes
Reducing or temporarily avoiding movements that aggravate symptoms is often the first step. Shifting to low‑impact activities like cycling, walking on level surfaces, or swimming can maintain fitness while allowing tissues to heal. Weight management also helps decrease load on the hip joint.
Medications
Short‑term use of nonsteroidal anti‑inflammatory drugs (NSAIDs) or acetaminophen can reduce pain and inflammation for many hip conditions. In some cases, physicians may prescribe stronger analgesics, neuropathic pain medications, or topical agents.
Targeted Physical Therapy
Physical therapy is central to conservative treatment for most non‑arthritic and arthritic hip problems. Programs typically include:
- Strengthening of hip, gluteal, and core muscles.
- Stretching tight muscles and tendons.
- Gait and movement retraining to reduce abnormal loads.
- Home exercise programs tailored to patient goals.
For non‑arthritic hip pain (like FAI and labral pathology), non‑operative management that combines patient education, activity modification, and individualized exercises can reduce pain and improve function in many patients.
Injections and Image‑Guided Procedures
Corticosteroid injections into the hip joint or bursae may offer significant but time‑limited relief for arthritis, bursitis, or inflammatory flares. In select cases, platelet‑rich plasma (PRP) or other biologic injections may be considered, though evidence varies.

What Is the Prognosis with Non‑Surgical Care?
Outcomes depend on the underlying diagnosis, but many patients improve without surgery:
- A systematic review found that about 54% of patients with non‑arthritic hip‑related pain reported satisfactory response to non‑operative treatment.
- For FAI and similar conditions, structured conservative programs focusing on activity modification and physical therapy have shown meaningful improvements in pain and function for many patients over 12–24 months.
- Soft‑tissue problems such as bursitis, tendonitis, and mild strains often improve over weeks to a few months with appropriate rest, medication, and rehabilitation.
- Hip osteoarthritis is chronic, but multimodal non‑surgical management (exercise, weight reduction, medications, and injections) can delay or reduce the need for joint replacement in many individuals.
Early evaluation and a comprehensive, personalized treatment plan generally improve the likelihood of avoiding or postponing surgery and maintaining function.
Frequently Asked Questions About Hip Pain
Is hip pain just a normal part of getting older?
Hip pain becomes more common with age, but it is not “normal” to have persistent pain that limits daily activities; evaluation is recommended if symptoms last more than a few weeks or worsen.
When should I see a doctor for hip pain?
Seek care if pain lasts longer than 2–6 weeks, interferes with walking, sleep, or work, or appears suddenly after a fall; emergency care is needed for inability to bear weight or suspected fracture or infection.
Does all hip pain mean I have arthritis?
No; many conditions including bursitis, tendon injuries, labral tears, stress fractures, and referred spine pain can mimic arthritis.
Can hip pain improve without surgery?
Yes; a large proportion of non‑arthritic hip conditions respond to non‑operative care, and many people with early arthritis manage well for years with conservative treatment.
What exercises are safe if I have hip pain?
Low‑impact activities like walking on flat surfaces, cycling, and swimming are generally safe, especially when supervised by a physical therapist who can tailor exercises to your condition.
Are steroid injections safe, and how long do they last?
Yes; weight loss, increased physical activity, and targeted exercise programs have strong evidence for reducing hip pain and improving function in both non‑arthritic and arthritic conditions.
How do I know if my hip pain is coming from my back?
Can lifestyle changes really make a difference?
Regain Your Hip Strength With Holistiq
If hip pain is limiting your movement, sleep, or quality of life, you don’t have to wait for it to “go away on its own.” A focused evaluation and personalized non‑surgical plan—built around your goals and daily activities—can often relieve pain, restore function, and help you stay active for years to come.
Where Does It Hurt? We Can Help.


Hip Pain
- Hip Pain Overview
- Avascular Necrosis
- Bursitis
- Gluteal Tendinopathy
- Pain by Activity (Walking, Running, Sitting, Sleeping)
- Pain in Athletes
- Pain in Older Adults
- Pain by Location (Front, Side, Rear)
- Iliopsoas Pain
- Impingement Syndrome
- Labral Tear
- Osteoarthritis
- Pain After Hip Replacement
- Piriformis Syndrome
- Snapping Hip Syndrome